America’s healthcare system is running on fumes. You've heard the headlines about the nursing shortage and the burnout. But the real story isn't just that people are quitting. It’s that the way we train new workers is stuck in 1995. Adtalem Global Education, the massive parent company behind institutions like Ross University School of Medicine and Chamberlain University, is currently trying to fix a broken pipeline by essentially rebuilding it from the ground up.
The numbers are pretty grim. The Association of American Medical Colleges (AAMC) projects a shortage of up to 86,000 physicians by 2036. If you think that’s bad, look at nursing. We’re staring down a deficit of hundreds of thousands of registered nurses within the next few years. This isn't just a "help wanted" sign in a window. It’s a systemic collapse of the workforce that supports every hospital and clinic in the country. Don't forget to check out our recent article on this related article.
Most traditional universities can’t keep up. They have limited clinical spots and rigid schedules. They’re often disconnected from what a rural hospital in mid-America actually needs. Adtalem is leaning into a different model. They’re focusing on scale and speed without—theoretically—sacrificing the quality of the clinicians they pump into the system. It’s a high-stakes bet on whether private education can save public health.
Why traditional med schools are failing the workforce
Traditional academic medicine is prestigious, but it’s also exclusive to a fault. Thousands of qualified applicants get rejected every year simply because there aren't enough chairs in the lecture halls or enough rotations in the local teaching hospital. That’s a bottleneck we can’t afford. If you want more about the background here, National Institutes of Health provides an excellent summary.
Adtalem’s approach focuses on access. By operating schools like American University of the Caribbean School of Medicine (AUC), they tap into a pool of students who are capable but might have been overlooked by the Ivy League-style gatekeeping of U.S.-based institutions. These students often end up in "high-need" areas. I’m talking about primary care, internal medicine, and pediatrics. These aren't the flashy, high-margin surgical specialties that make TV shows popular. They're the front lines of keeping people alive.
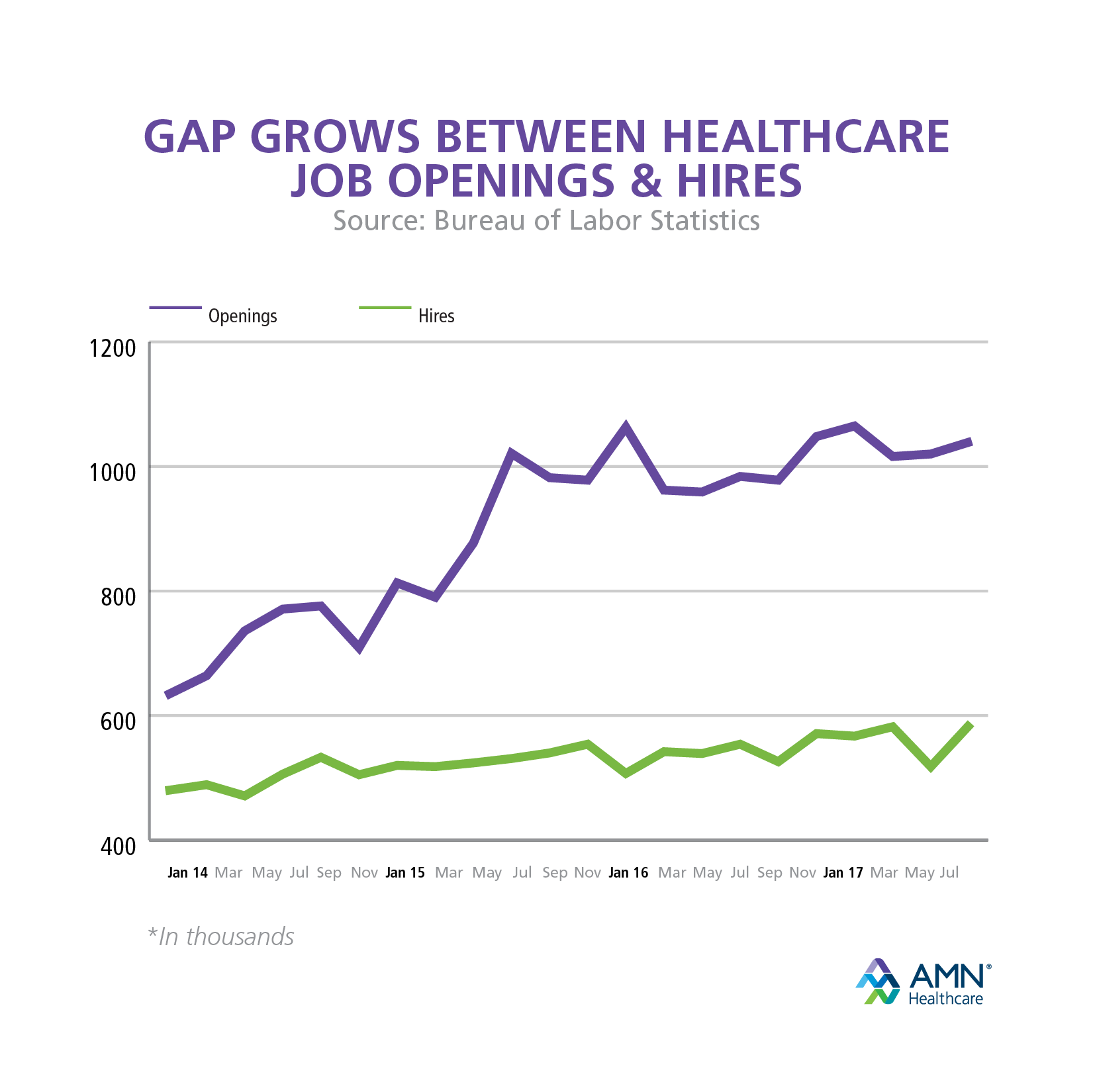
The "jobs gap" isn't just about a lack of bodies. It’s about a lack of the right bodies in the right places. If every new doctor becomes a plastic surgeon in Beverly Hills, the shortage in rural Iowa stays the same. Adtalem’s data suggests their graduates are far more likely to practice in underserved communities. That’s a huge deal for equity.
Clinical partnerships are the new currency
You can’t learn to be a nurse from a textbook or a Zoom call. You need hands-on time with patients. This is where the whole system usually grinds to a halt. Hospitals are short-staffed, so they don’t have enough mentors to take on students. It’s a vicious cycle.
To break this, large education providers are signing massive partnership deals with healthcare systems. They aren't just sending students there; they're co-designing the curriculum. They’re asking hospital CEOs, "What are your new hires missing?" and then baking those skills into the semester.
This model turns the hospital from a passive host into an active participant in the supply chain. Chamberlain University, for example, has worked with systems like LCMC Health to create tuition-free programs for employees. The hospital pays the bill, the school provides the training, and the student commits to working at that hospital for a set period. It’s a "grow-your-own" strategy that actually works.
Diversity as a survival strategy
If your medical staff doesn't look like the community it serves, patients get worse care. It’s a fact. Studies consistently show that patient outcomes improve when there’s a shared cultural understanding between the provider and the person on the exam table.
Adtalem claims to be one of the largest producers of diverse healthcare professionals in the U.S. This isn't just about checking boxes for a PR slide deck. It’s about survival. A workforce that only draws from the top 10% of wealthy zip codes will never be large enough to fill the gap. We need talent from everywhere—first-generation students, career changers, and people from the very neighborhoods that are currently "healthcare deserts."
When you look at the graduation rates for Black and Latino doctors from these large-scale private institutions, they often outpace traditional state schools. We have to stop looking at these "non-traditional" pathways as secondary. They’re becoming the primary engine for diversity in the field.
The tech shift that isn't just hype
Forget the buzzwords. The actual tech change happening in healthcare education is about simulation. High-fidelity mannequins that bleed, sweat, and go into cardiac arrest are replacing some of the early-stage "trial and error" on real humans.
This allows schools to scale. You can run 50 students through a complex birthing simulation in a weekend. You can’t do that in a real labor and delivery ward without causing chaos. It speeds up the "competency" clock. Instead of waiting for a specific rare case to walk through the ER doors, the school can force the student to handle it in a controlled environment.
But there's a catch. Tech costs money. This is why the big players are winning. A small nursing school at a local community college might not have the budget for a $100,000 "SimMan" or a virtual reality anatomy lab. The consolidation of healthcare education is happening because the barrier to entry—the cost of modern training tools—is skyrocketing.
The burnout factor nobody wants to talk about
We can train a million new nurses, but if the work environment is toxic, they’ll leave in six months. This is the "leaky bucket" problem. Adtalem and its peers are trying to address this by adding "resilience training" and mental health support into the curriculum.
Honestly, that’s a bit of a band-aid. The real fix has to happen in the hospitals. However, by preparing students for the reality of a high-stress environment—rather than a sanitized version of it—these schools hope to reduce the "reality shock" that leads to early turnover.
We’re also seeing a shift toward more flexible learning models. Many of these students are working adults. They have kids. They have mortgages. The old-school model of "sit in a lecture from 8 to 5" is dead. If we don’t make education fit into a messy, busy life, we lose half the potential workforce before they even start.
What needs to happen next
If you're a healthcare leader or a policy maker, the "jobs gap" should be your top priority. But stop looking for a single magic bullet. It’s a multi-front war.
- Standardize clinical spots: States need to offer tax incentives to hospitals that prioritize hosting students. We need to make it more profitable to teach than to not teach.
- Expand the scope of practice: We need to let Nurse Practitioners and Physician Assistants do more. If they’re trained at a high level, let them use that training. This offloads the burden from overworked MDs.
- Fund the "middle": We focus a lot on doctors and nurses. We forget about respiratory therapists, lab techs, and radiologic technologists. These roles are just as empty and just as vital.
- Embrace the scale: Stop the snobbery around large-scale education providers. If they’re meeting accreditation standards and their students are passing board exams, they are a vital part of the solution.
The gap isn't going to close itself. We’re currently in a race between a declining workforce and a rising elderly population. Right now, the elderly are winning. The only way to flip the script is to change how we define, fund, and deliver medical education. It’s messy, it’s expensive, and it’s absolutely necessary.
Check the accreditation and "match" rates of any program you’re considering. Don't just look at the brand name. Look at the data. If a school isn't transparent about how many of their students actually get jobs, walk away. The stakes are too high for anything less than total transparency.